Understanding Kyle Korver’s Injury: A Complete Primer to Ankle Injuries
- Post By: Jeff Stotts
- Date:
- Category: NBA, Understanding...
ACL tears are devastating and concussions are the rightful hot topic in sports. However neither injury has dominated the NBA like the ankle sprain. Nearly every player from every era has felt the pain of a turn, tweak, or twist of the joint. An ankle sprain was one of the few injuries to sideline Michael Jordan for a game during his run with the Bulls and was the culprit behind LeBron James’ first missed games as a professional. No other injury lights up the InStreetClothes.com database with over 1,800 ankle sprains recorded. The injury reared its ugly head again last night when Hawks’ forward Kyle Korver had his right ankle roll inward following a collison with Cleveland’s Matthew Dellavedova.
Official release on Hawks G Kyle Korver out for the rest of the season with a severe high right ankle sprain: pic.twitter.com/X6SSrGu6bW
— Jeff Zillgitt (@JeffZillgitt) May 23, 2015
Sadly the injury will end Korver’s 2014-15 season and surgery is currently being considered. Understanding ankle injuries can be difficult but here is the InStreetClothes.com ankle injury primer.
Forming the Ankle
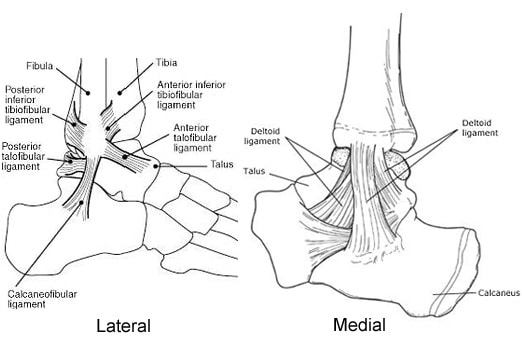
Anatomically the ankle joint appears quite simple. It’s comprised of the three bones, the tibia and fibula of the lower leg and the talus of the foot. However the ankle as a functional unit is actually made up of three different joints.
The first is the talocrural joint or the “true” ankle joint. It is formed from all three aforementioned bones and is involved with the up and down movement known as plantar flexion and dorsiflexion. Ligaments located on both sides of the leg and foot stabilize this area. On the inside, or medial aspect, of the ankle is the strong deltoid ligament that prevents excessive inward movement or eversion. Three additional ligaments are located on the lateral or outside of the ankle. These ligaments, the anterior talofibular ligament (ATFL), the posterior talofibular ligament (PTFL), and the calcaneofibular ligament, (CFL) are the most vulnerable to injury and are sprained while the ankle is forced into inversion following an awkward step or when landing on the foot of another player.
The next joint involved in the ankle is the subtalar joint and is formed between the talus and the calcaneus. Here the motions of inversion and eversion are made possible. Like the talocrural joint, ligaments fortify the subtalar joint.
The final joint included in the ankle is the distal tibiofibular joint. It is located at the bottom of the leg, where the tibia and fibula join with the talus. A strong ligament known as the interosseous ligament stretches across the joint to connect the two lower leg bones while two additional ligaments, the anterior and posterior tibiofibular ligaments, assist in stabilizing the ankle mortise. Any injury that occurs to these ligaments is classified as a “high ankle” or syndesmotic sprain.
Grading Injuries
The ligaments of the body connect bone to bone. To allow for mobility and stability, ligaments have inherent viscoelastic characteristics that allow them to be both viscous and elastic. Simply put, a ligament can withstand an applied stress by rearranging its basic makeup to better provide stability. However each ligament has a very specific yield point and failure point. When the amount of stress pushes a ligament beyond its yield point, a sprain occurs. Microtrauma to the fibers that make up the ligament is considered a mild or Grade I ankle sprain. Basically the ligament has been overstretched but remains intact as a whole. Players with Grade I sprains may not even miss a game.
A Grade II sprain occurs when particular fibers of the ligament fail and is often referred to as a moderate sprain or a partial tear. Grade II sprains are generally more painful and limiting. The associated symptoms are more severe with high amounts of swelling usually occurring. As a result these injuries require intensive treatment and extended rest.
Finally a Grade III sprain is a crippling and severe injury. These injuries result in a total loss of function and stability. Grade III sprains often require a considerable amount of rest and in some rare cases surgery.
Furthermore, Grade II or III sprains are more likely to have long-term ramifications, primarily on the stability of the affected joint and the likelihood of reoccurrence. In these injuries, the ligaments have passed their yield point. Once this has occurred, its strength and integrity remains forever altered. The concept is similar to a rubber band. When a rubber band is new and fresh from the package it is stretchy yet strong. As it is used over and over again, the rubber band is slowly worn down, moving past its yield point. The once strong rubber band becomes stretched out, decreases in strength, and loses its elasticity. A sprained ligament acts in similar fashion. Once a ligament has been stressed past its yield point its physical makeup remains perpetually effected, though various treatments and rehab protocols can return the ankle close to its original state. Still once an ankle has been sprained it remains more susceptible to being aggravated and re-sprained.
Accompanying Injuries
Sprains rarely occur in an isolated manner. The violent nature of the injury often includes damage to neighboring structures. Strains to the muscles of the ankle are common with a sprain as the involved tendons are also overstretched. Injuries to bone are another regular occurrence.
Avulsion fractures frequently accompany medial ankle injuries as the deltoid ligament pulls away a small piece of bone. A bone contusion or bone bruise can occur if the stress of the incident causes damage to the outer layer of one of the involved bones. The injuries are not as severe as a fracture but require additional time to heal. The body’s recovery response treats bone bruises just like a fracture filling in the damaged area with new bony tissue.
Recovery and Rehab
The timeline of recovery widely varies based on the severity of damage, the involved tissues, and a multitude of other variables. Generally speaking the first phase of recovery involves controlling the associated symptoms like swelling and pain. An injured player may be placed on crutches or immobilized in a walking boot to minimize the amount of weight placed on and through the injured joint. A progressive rehab protocol can be initiated once the medical professional involved feels the player is ready. The preliminary focus of rehab is on regaining and retaining range of motion. The next step concentrates on strengthening the area and insuring proper muscle function. Finally the athlete will transition to basketball specific drills. Additional work on lateral movement is often necessary to assure the ligaments are capable of withstanding the applied stress.
Again Korver’s ankle injury appears to have occurred on the inside portion of the joint when the ankle was forced into eversion. The Hawks official press release also indicates the injury contains components of a high ankle sprain. Korver will visit with specialists before determining a final course of treatment. Unfortunately the All-Star forward becomes just the latest player to go down with an injury during this year’s postseason, joining a list that includes Los Angeles Clippers guard, Cleveland forward Kevin Love, and Washington guard John Wall.
[…] Read it here: http://instreetclothes.com/2015/05/23/understanding-kyle-korvers-injury-a-complete-primer-to-ankle-i… […]